
By Chloe (Jin Ying) Liu and Zan Ding
Introduction
Tuberculosis is a disease caused by bacteria called Mycobacterium tuberculosis. This kind of bacteria usually attacks the lungs, but it can also influence other parts of the body such as the brain, kidney or spine. If a person is infected with tuberculosis, the general symptoms include feelings of sickness or weakness, weight loss, fever and night sweats. Besides, the symptoms of tuberculosis on the lungs include coughing, chest pain, and the coughing up of blood. Tuberculosis bacteria can stay in the air for several hours (1) and be easily spread through coughing, sneezing, talking, or singing.
Mycobacterium tuberculosis
Mycobacterium tuberculosis has ropelike structures of peptidoglycans that give it properties of an acid fast bacteria. It is able to form acid-stable complexes when certain arylmethane dyes are added (2). M. tuberculosis has circular chromosomes of about 4,200,000 nucleotides long. Plasmids in M. tuberculosis are important in transferring virulence because genes on the plasmids are more easily transferred than genes located on the chromosomes (2). The tough cell wall of the bacteria with unusual structure and composition prevents passage of nutrients into and out of the cell, therefore M. tuberculosis grows slowly.
Figure 1: How TB Spreads. Source: http://www.cdc.gov/tb/topic/basics/default.htm.
Tuberculosis outbreak
Most tuberculosis cases do not start outbreaks, however they do occur and they can put tremendous strain on local public health resources. All outbreaks begin with a source case. Recognizing the characteristics of such patients soon after diagnosis could help to interrupt transmission and reduce the risk for an outbreak. There were nonrandom outbreaks of TB in the United States during 2002-2008, which the Centers for Disease Control and Prevention (CDC) assisted in investigation. Outbreaks are defined based on CDC guidelines for contact investigation as detection of tuberculosis disease between more than two people exposed to a person with infectious tuberculosis (5). From this review, the outbreak in the United States had more than 3 culture-confirmed cases that had epidemiologic links and tuberculosis strains with matching genotypes. Linkage by epidemiology means exposure to another outbreak patient by sharing enclosed airspace in the same period. Genotyping methods included spoligotyping and either restriction fragment length polymorphism ore 12-locus mycobacterial interspersed repetitive units. Of the 51 tuberculosis investigations during 2002-2008, a total of 27 met the defining criteria, while 24 cases were excluded because some of these cases include patients with organ transplants and some had insufficient data in CDC reports. Based on the study of this outbreak in the United States, about 84% of patients had pulmonary disease; 25% of patients required hospitalization and 6% died.

Figure 2: Characteristics of source case-patients for 26 investigated tuberculosis outbreaks, United States, 2002–2011. Source: http://wwwnc.cdc.gov/eid/article/21/3/14-1475-t1.
Causes of outbreaks
Factors contributed to outbreak include delays in seeking medical attention which may cause intense transmission. The infectious period for pulmonary tuberculosis cases was assumed to start three months before tuberculosis symptoms onset and to end with the initiation of tuberculosis (4). Outbreak duration is calculated beginning on the treatment start date for the first reported case and continuing through treatment start date for the last case as noted at the time of the investigation. Prolonged infectious period was defined as more than three months between symptom onset and the date that effective treatment had been administered for two weeks (5). Educating health care providers in order to raise public awareness about tuberculosis is critical. In this way, patients can seek early diagnosis and receive timely treatment which results in efficient control of potential TB transmission.
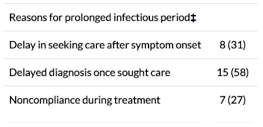
Figure 3: Characteristics of source case-patients for 26 investigated tuberculosis outbreaks, United States, 2002–2011. Source: http://wwwnc.cdc.gov/eid/article/21/3/14-1475-t1
When contact investigations are incomplete because of limited resources or hard-to-reach populations, latent tuberculosis infection remains so that TB outbreaks can spread. Identifying high-risk settings is another basic principle of tuberculosis control except applying effective control measures to reduce TB transmission. TB outbreak hotspot was the drug house. According to the data, about 63% of cases were occurred there. Homeless shelters, correctional facility, household, workplace, church, bar, school and public transit were common places for TB outbreak. The most frequently intervention to manage the outbreak is to prioritize contacts based on risk for infection and progression of disease, enabling the highest risk contacts to be completely evaluated.
Tuberculosis disease can be treated by using antibodies to kill the bacteria M. tuberculosis. Isoniazid (INF) and rifampin (RIF) are most commonly used antibodies in the treatment(6). Effective treatment is difficult and prolonged to achieve because of unusual mycobacterial cell wall, taking 6 – 9 months. Although therapeutic effects have accomplished and TB incidence has declined in the United States, public health departments still require more efficient strategies to prevent, detect, and treat TB in order to eliminate the disease fundamentally.
Reference:
- TB Elimination Tuberculosis: General Information. (n.d.). Retrieved November 3, 2015, from http://www.cdc.gov/tb/publications/factsheets/general/tb.pdf
- Uhía, I., Galán, B., Medrano, F. J. & García, J. L. Characterization of the KstR-dependent promoter of the gene for the first step of the cholesterol degradative pathway in Mycobacterium smegmatis. Microbiology 157, 2670 (2011)
- Mitruka K, Oeltmann JE, Ijaz K, Haddad MB. Tuberculosis outbreak investigations in the United States, 2002–2008. Emerg Infect Dis. 2011;17:425–31. DOIPubMed
- Centers for Disease Control and Prevention. Guidelines for the investigation of contacts of persons with infectious tuberculosis. Recommendations from the National Tuberculosis Controllers Association and CDC. MMWR Recomm Rep. 2005;54(RR-15):1–47 .PubMed
- Centers for Disease Control and Prevention Guidelines for the investigation of contacts of persons with infectious tuberculosis: recommendations from the National Tuberculosis Controllers Association and CDC. MMWR Morb Mortal Wkly Rep. 2005;54(RR–15):1–3 [PubMed]
- Core Curriculum on Tuberculosis: What the Clinician Should Know (5th ed.). Retrieved June 21, 2013, from http://www.cdc.gov/tb/education/corecurr/pdf/corecurr_all.pdf
