
by Kevin Xue
Introduction:
When Alexander Fleming discovered penicillin in 1928, the modern world aspired to finally be rid of bacterial associated diseases. The effect of antibiotics had such a significant impact on public health that deaths by pathogenic bacteria declined significantly and a simple prescription of antibiotics would be an automatic and casual response. Unfortunately, this illusion was quickly shattered as bacterial infections started causing more illnesses and deaths again around the 1950s. Staphylococcus aureus (S. aureus), having acquired resistance to the beta-lactam class of antibiotics, is one of the most significant species of bacteria responsible for the re-emergence of bacterial disease. The beta-lactam class encompasses the family of drugs with the same mode of action as penicillin. Consequently, the concept of the “superbug” Methicillin-Resistant S. aureus (MRSA) has become widely feared.
History of MRSA:
Resistance to penicillin dates as far back as 1942. Just about ten years later, roughly 70% of S. aureus isolates could deal with penicillin. With the increase of untreatable cases, a new derivative of beta-lactams referred to as methicillin was released for use in 1961. The optimism surrounding this new drug rapidly vanished as resistance was reported only a year after its implementation. The frequency of resistance to the drug escalated quickly as strains that could survive methicillin escalated from 0.1% to 75% frequency in just 40 years (Figure 1). Though MRSA has been historically found in hospital settings, community acquired strains (CA-MRSA) have recently begun to emerge. Some of these strains such as the notable USA300 and USA500 account for most cases of community acquired strains.
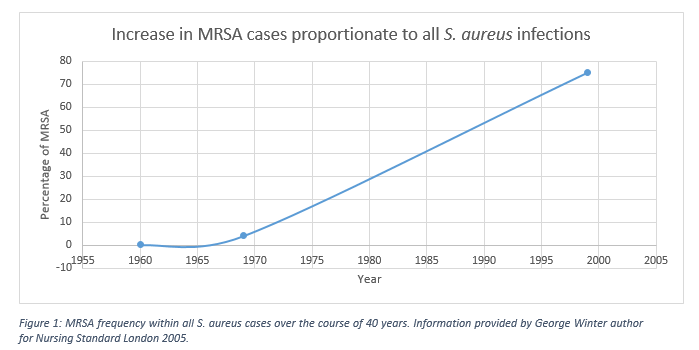
Figure 1: MRSA frequency within all S. aureus cases over the course of 40 years. Adapted from George Winter, Nursing Standard London, 2005.
The rise of antibiotic resistance:
In microbiology, any given population of bacteria will typically experience relative genetic diversity. Sometimes it takes just a small change in their genome for a bacterium to become resistant to antibiotics. Practically speaking, spontaneous resistance to antibiotics at an individual level happens very rarely in normal conditions. On the other hand, if resistant cells are selected for, then large scale resistance can occur as non-resistant strains perish and give way to their more adapted albeit it, fewer counterparts. Moreover, resistance to a drug can often depend on its dosage. If an infected person takes an antibiotic but does not consume the full treatment course, there may be a chance that mildly resistant bacteria survive treatment. The rise of resistance does not occur only in pathogens, normal bacterial populations that harmlessly inhabit animals can develop resistance also. Alternatively, non-infectious bacteria with antibiotic resistance can exchange DNA with pathogenic bacteria and confer resistance (Figure 2).
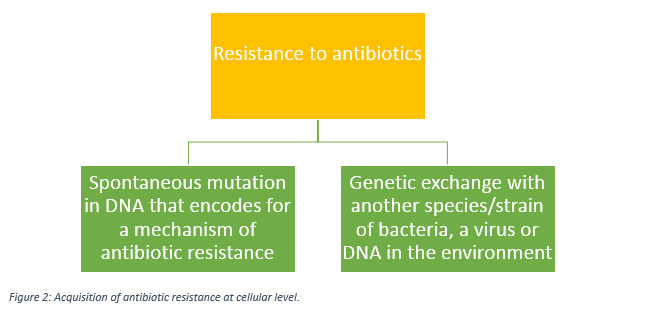
Figure 2: Acquisition of antibiotic resistance at cellular level.
If antibiotic treatment is improperly prescribed to a patient in a singular case, the consequences are minimal provided that the patient follow the treatment properly. Contrarily, if antibiotics are prescribed to millions of people, the pool of resistant bacteria will keep expanding assuming a portion of the patients forego the rest of the treatment after clearance of symptoms and the partly resistant bacteria are allowed to grow again. Thus many factors can give rise to pools of antibiotic resistant bacteria. In practise, the overall rate of antibiotic strain diversity in MRSA is correlated with the overall antibiotic prescription policy and hospital regulation of a given region. In essence, the liberal use of antibiotics and the poor adherence to treatment by patients have greatly accelerated resistance in bacteria (Figure 3).
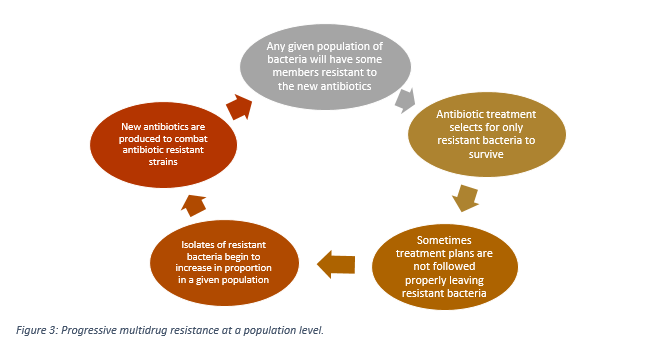
Figure 3: Progressive multidrug resistance at a population level.
Transmission and Pathogenicity:
The literature seems to agree that roughly 30% of people will have their nasal passages colonized with S. aureus. In England, estimates of about 1.5% of people carry MRSA. Though formerly believed to be transmitted by skin to skin contact, it appears that fomites may act as a source of transmission also. Fomites consists of objects and surfaces on which bacteria can survive or grow and can include anything from hospital beddings to cellphones. Once colonized by MRSA, they become a risk factor for possible bacteremia or blood infection caused by a breach in skin. In less severe cases, skin infections can occur due to mucous membrane or skin breaching. Reports show nearly 80% of S. aureus infections are from the same strains found on the individual prior to actual infection, suggesting that asymptomatic colonization of MRSA is a risk factor.
Unfortunately, new strains of community acquired MRSA have been appearing frequently in the USA and can release a toxin called the Panton-Valentine Leukocidin (PVL) that targets host immune cells. These strains have been designated names such as USA300, USA400 and USA500. The PVL toxin allows MRSA to kill patients rapidly through necrotizing pneumonia (destruction of lung tissue) severe sepsis (causes whole body inflammation), and necrotizing fasciitis (skin-eating disease). CA-MRSA differ from hospital acquired strains as they tend to transmit through less traditional routes, such as via unprotected sex between men. As it stands, USA300 and similar strains appear to be especially dangerous due to new virulent traits that they have acquired.
Solutions:
Unfortunately, MRSA does not have many treatment options at the moment. When S. aureus first became methicillin resistant, the medical community started to realize that many of these bacteria were developing resistance to beta-lactams, which kills bacteria by preventing bacteria cell wall formation. As a result of beta-lactam resistance, research is being done on new modes of action for new antibiotics. Currently, vancomycin is being used as the main drug for MRSA. Unfortunately, vancomycin acts slowly and penetrates lung tissue poorly and thus MRSA related mortality still remains quite high. Additionally, vancomycin treatment selects for another dangerous pathogen resulting in vancomycin-resistant Enterococcus. As a species, S. aureus can be considered to be resistant to nearly all antibiotics. It is important to remember that antibiotics that have been rarely used are likely effective against most strains of MRSA as resistant ones would be selected for infrequently. As a result, many of the older and possibly more harmful antibiotics such as tetracycline and clindamycin are still effective. Moreover, by combining multiple antibiotics in a treatment, the probability of an MRSA strain resistant to all of the drugs plummets. Theoretically, MRSA can keep developing resistance until the point where one strain may be untreatable. Ultimately, vigilant and tight control on antibiotic treatment plans will help reduce selective pressure leading to fewer cases of strains surviving any single treatment.
Final considerations:
Though antibiotics can be viewed as a “god-sent” solution to the numerous pathogens that have ravaged the human population throughout history, it is important to keep in mind that life can adapt provided there is enough room to work with. MRSA represents a painful wakeup call. The poorly managed use of antibiotics has provided ample opportunity for this pathogen to rapidly become a superbug. In the future, caution and thought must be taken to insure that solutions to disease related problems do not create new problems.
References:
Banning, M. (2005). Transmission and epidemiology of MRSA: current perspectives. British Journal of Nursing 14:30 548-554.
Baddour, M.M. (2010) MRSA infections and treatment. Nova Science Publishers Inc., New York.
Bush, K. (2015) Synergistic MRSA combinations. Nature Chemical Biology 11, 832-833.
Byrne, F.M., Wilcox, M.H. (2011) MRSA prevention strategies and current guidelines. Injury Int. J. Care Injured 42, S3-S6.
Decker, C.F. (2008) Pathogenesis of MRSA infections. Disease-a-Month 54:12, 774-779.
Lubowitz, J.H., Poehling, G.G. (2008) Methicillin-Resistant Staphylococcus aureus. Arthroscopy : The Journal of Arthroscopic & Related Surgery 24:5, 497-499.
Tenover, F.C., Mcdougal, L.K., Goering, R.V., Killgore, G., Projan, S.J., Patel, J.B., Dunman, P.M. (2006) Characterization of a Strain of Community Associated Methicillin-Resistant Staphylococcus aureus Widely Disseminated in The United States. J. Clin. Microbiol 44:1, 108-118.
Winter, G. (2005) Origin of the Species The rise of antibiotic resistance and MRSA. Nursing Standard London 19:34: 24-25.
