
by Fahima Ahmed, Christina Ghaly, Kathia Farah, and Bailey Jarrett
INTRODUCTION
Bartonella quintana is a pathogenic microorganism that is the causative agent of Trench Fever. Found in clothes and associated with poor hygiene, poverty and cold weather, this bacterium multiplies in the intestine of a louse (a small wingless parasitic insect) and is excreted in its feces. It is then transmitted by blood-suckling lice on the human body (Pediculus humanus). The pathogen is able to grow in red blood cells, and may result in chronic bacteremia if the individual is immunocompetent.
DISEASE
The vector-borne disease is characterized by fever, headaches, shin pain and dizziness, caused by destruction of the red blood cells. Transmission to humans occurs through contact of the excrement with breaks in the skin. The lice inject proteins that induce scratching, making fecal transmission easier. B. quintana adheres to the epithelium and endothelium, which is a tissue made of a single layer of cells that line the heart, blood and lymph vessels, and invades erythrocytes. Clinical manifestations of this disease range from asymptomatic infection to severe illness. The lipopolysaccharide (a large molecule consisting of a lipid and sugar on the surface of Gram-negative bacteria) of this pathogen was shown to down-regulate the action of immune cells and pro-inflammatory cytokines, resulting in the absence of symptoms usually manifested during bacteremia (the presence of bacteria in the blood). However, when the bacterium remains in the blood persistently, years after the initial infection, it results in chronic bacteremia, as well as disruption and inflammation of vascular tissues.
EPIDEMIOLOGY
Bartonella quintana was first identified as a human pathogen during World War I, when it caused an epidemic of Trench Fever among one million soldiers in Europe. B. quintana is now found worldwide and causes febrile outbreaks (symptoms of a fever), although infected people regularly recover. It is most commonly recognized as a disease among the homeless population in the United States and Europe. This is because poor sanitation, personal hygiene and alcoholism increase its transmission rate. In France, 30% of 71 tested homeless people had a high concentration of antibodies against B. quintana, with 14% that were bacteremic. In Seattle, 20% of low income patients had antibody titers for B. quintana of 1:64 or greater, meaning there is evidence of recent or current infection. A severe form of B. quintana has also been reported in immunocompromised patients, such as those with AIDS.
VIRULENCE
Bartonella quintana infects red blood cells in a stepwise fashion as shown below.
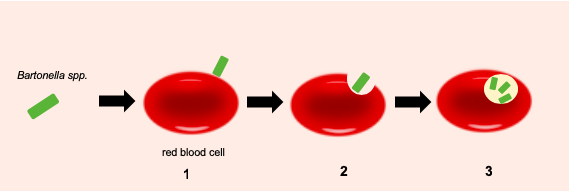
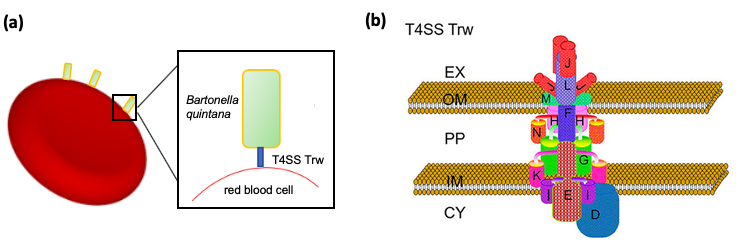
B. quintana uses multiple virulence factors to infect red blood cells. The type-IV secretion system (T4SS) is the most important one. T4SS are made up of proteins that form a channel across the membranes of bacteria. Through this channel, bacteria can transfer toxins, DNA plasmids or proteins directly into the cytoplasm of recipient cells. The system mediates intimate contact with host cells. The T4SS of B. quintana, called Trw, is necessary for erythrocyte infection, although its function as a secretion system is not clear. However, the role of the Trw in adhesion of RBCs is well-known. Trw has multiple copies of two surface-exposed subunits, TrwL and TrwJ (seen in Figure 2 (b)). These components help to recognize and bind specifically to erythrocyte receptors on the cellular membrane. The virulence factor is therefore responsible for the specificity of host cells it infects. The Trw initiates attachment to RBCs while other virulence factors are used for further adherence and invasion. For example, variable outer-membrane proteins (VOMPs) bind to the components of the extracellular matrix of the host, such as fibronectin and collagen, and allow entry of the pathogen into RBCs.
Once in the cytoplasm, the bacteria proliferates inside a vacuole that supports its growth. The pathogen also acquires nutrients from the host by using hemin-binding protein (that bind to hemin found in hemoglobin of human blood) and other proteins involved in amino acid nutrient uptake. B. quintana stays inside for the lifetime of erythrocytes, increasing the likelihood of transmission by blood-sucking vectors.
TREATMENT
The choice of antibiotic therapy for B. quintana infection is problematic. A lot of antibiotics cannot reach intracellular bacteria since they cannot cross the host cell membrane, making them unable to treat the infection effectively.
Randomized trials on affected patients have shown an eradication following a doxycycline and gentamicin treatment, when given together. Doxycycline is capable of intracellular penetration and will stop the growth of the bacteria.
A benefit from aminoglycoside therapy was also suggested following treatment for patients with endocarditis. Patients who received a regimen that included at least 14 days of an aminoglycoside had a greater likelihood of achieving full recovery and surviving the infection, as opposed to those treated only with doxycycline.
REFERENCES
Angelakis, E., Raoult, D. (2014) Bartonellosis, Cat-scratch Disease, Trench Fever, Human Ehrlichiosis. In Manson’s Tropical Infectious Diseases, 23, 385-394.
Brouqui, P., Doudier, B. (2013) Trench Fever. In Hunter’s Tropical Medicine and Emerging Infectious Disease, 9, 561-563.
Brouqui, P., Dolan, M. J., Koehler, J. E., Maguina, C., Raoult, D., Rolain, J. M. (2004) Recommendations for Treatment of Human Infections Caused by Bartonella Species. In Antimicrobial Agents and Chemotherapy, 48(6), 1921-33. doi: 10.1128/AAC.48.6.1921-1933.2004
Brouqui, P., Foucault, C., Raoult, D. (2006) Bartonella quintana Characteristics and Clinical Management. In Emerging Infectious Disease, 12(2), 217-223.
Cohn, J., Mazo, D., Mosepele, M. (2012) Bartonella Infection in Immunocompromised Hosts: Immunology of Vascular Infection and Vasoproliferation. In Clinical and Developmental Immunology 2012, 612809.
Deng H., Pang Q., Zhao B., Vayssier-Taussat M. (2018) Molecular mechanisms of Bartonella and mammalian erythrocyte interactions: a review. In Frontier Cellular Infection Microbiology, 8, 431-442. doi: 10.3389/fcimb.2018.00431.
Harms A., Dehio C. (2012) Intruders below the radar: molecular pathogenesis of Bartonella spp. In Clinical Microbiology Reviews, 25(1) 42-78. doi: 10.1128/CMR.05009-11
Jackson, L. A., Spaeh, D. H., Kippen, D. A., Sugg, N. K., Regnery, R. L., Sayers, M. H., & Stamm, W. E. (1996). Seroprevalence to Bartonella quintana among Patients at a Community Clinic in Downtown Seattle. Journal of Infectious Diseases, 173(4), 1023–1026. doi: 10.1093/infdis/173.4.1023
Malgorzata-Miller, G. et al. (2016) Bartonella quintana lipopolysaccharide (LPS): structure and characteristics of a potent TLR4 antagonist for in-vitro and in-vivo applications. In Sci. Rep. 6, 34221. doi: 10.1038/srep34221
Maurin, M., Raoult, D. (1996) Bartonella (Rochalimaea) quintana infections. In Clinical Microbiology Reviews, 9(3), 273-92.
Maurin, M., & Raoult, D. (2001) Use of aminoglycosides in treatment of infections due to intracellular bacteria. In Antimicrobial agents and chemotherapy, 45(11), 2977–86. doi:10.1128/AAC.45.11.2977-2986.2001
Spach, D. (2019) Clinical features, diagnosis, and treatment of Bartonella quintana Infections. Retrieved from UpToDate.com/ https://www.uptodate.com/contents/clinical-features-diagnosis-and-treatment -of-bartonella-quintana-infections#references
