
by Tongzhu Meng and Luyang Yuan
Introduction:
Yersinia pestis, also used to be named as Bacterium pestis, Bacillus pestis and Pasteurella pestis, is the causative agent of plague, which is a disease primarily affecting rodents via their associated fleas and is able to transmit to humans through infectious fleabites. Y. pestis was thought to be responsible for three devastating pandemics throughout human history, including the Justinian’s plague during the 6th century, the Black Death in Europe and Modern plague in China in the later 19th century. The bacterium was discovered during the epidemic of the plague in Hong Kong and had been used as a biological weapon during the 20th century. Y. pestis can be found exclusively in mammalian hosts and arthropod vectors, such as fleas.
Disease:
Plague is a serious infectious disease that has three major clinical forms: bubonic plague, septicemic plague and pneumonic plague. If the patient is bitten by an infected flea, Y. pestis bypasses the skin barrier, enters the bloodstream and multiplies inside the lymph nodes. In healthy individuals, macrophages are guards of the immune system that are able to digest invading bacteria. Y. pestis inhibits macrophages from clearing bacteria and causes patients to have fever and one or more swollen lymph nodes. Y. pestis prevents local immune cells from eliminating bacteria and communicating with other remote immune cells that are able to help controlling the infection.
Septicemic plague can exist as the first symptom of plague or as secondary symptom of untreated bubonic plague. This form is the result of infectious fleabites or handling tissues or fluids of an infected animal. Under this kind of scenario, patients’ fingers, toes, the nose and other tissues might get black, due to reduced blood flow. They are also susceptible to develop bleeding into the skin and inner organs. Pneumonic plague is the result of inhaling infectious droplets in the air or from untreated bubonic or septicemic plague after the bacteria have spread to the lungs. It is the most serious form of the plague and is the only form of the disease that can be spread from person to person through infectious droplets. Infections of lung may lead to pneumonia and cause chest pain, respiratory failure and shock.

Figure 1: Summary of transmission process of Yersinia pestis to human. (by Tongzhu Meng)
Epidemiology:
From 2010 to 2015, WHO reported 3248 cases worldwide, including 584 deaths. Plague epidemics have occurred in Africa, Asia and South America, but since 1990s, most human cases reported were occurred in Africa. Nowadays, the three most vulnerable countries in the world are Democratic Republic of the Congo, Madagascar and Peru. Bubonic plague has a mortality rate of 30% to 60% while pneumonic plague is always fatal unless treatment started within 20 hours of symptom onset.
Over 80% of cases reported in United States were in bubonic form and there was an average of seven human plague cases reported each year for the past decades. These reported human cases covered people in all ages and in both sexes. Moreover, according to the cases reported in the last 20 years, people living in small towns and villages or agricultural areas are more susceptible than those living in larger towns and cities or urban areas.
Virulence Factor:
Y. pestis gets into the body by flea bites or by contaminated fluid or by infectious droplets in the air. Phagocytes, such as macrophages, are a type of cell that circulates in the body, which can engulf and digest bacteria and other non-self material. In healthy individuals, these cells would recognize bacteria and then engulf it by a process called phagocytosis. This leads to the formation of a bag of bacteria in the phagocyte, which is called phagosome. Then the enzymes located in the phagocytes are pumped into phagosomes to destroy the bacteria.
However, Y. pestis is resistant to phagocytosis. There are two important virulence factors contributing to this property named F1 (Fraction 1) and LcrV. LcrV may also play a role in suppressing the immune response in an individual, it could inhibit production of signal molecules released by immune cells that would lead to the silence of normal immune response. The bacteria are able to move in the circulation and travel to local lymph nodes. It is resistant to be digested by macrophage and it can replicate within the lymph nodes rapidly, which causes swelling and enlargement of the lymph nodes.
Y. pestis has a needle-like structure (Figure 2), which is necessary to infect the host cells. It injects secretory proteins produced by Yersinia into macrophages and other immune cells. Some of these secreted proteins form pores on the host cell membrane and lead to the destruction of the host cells. Those pores created by the secretory proteins serve as gates for the other secretory proteins to get into the cells. Some of these secretory proteins limit the ability of immune cells to engulf the bacteria and other non-self materials and affect the signaling pathway of the immune system. Moreover, some of them could get into the host cells and lead to the killing of the host.
To sum up, Y. pestis is resistant to phagocytosis. It causes the death of host cells and affects the signals between the immune cells in the host that leads to suppression of normal immune responses.
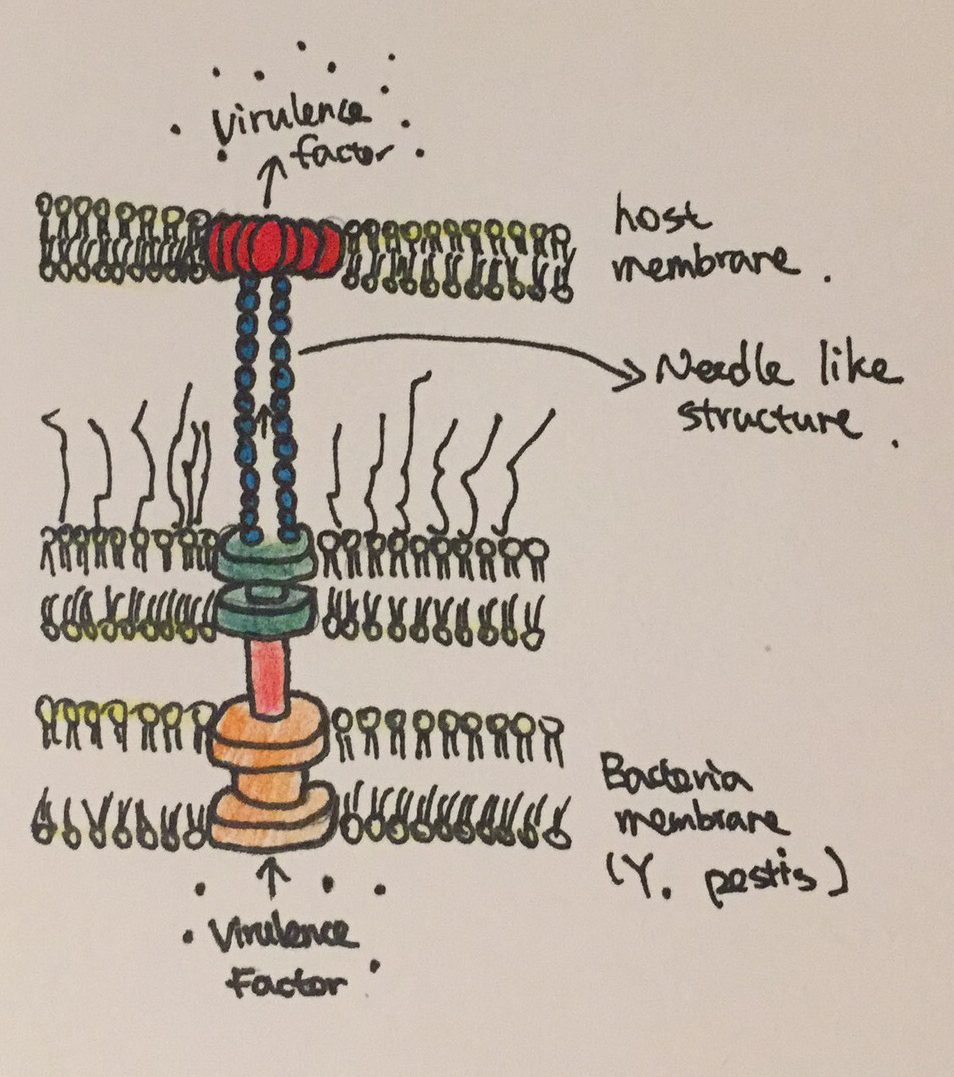 Figure 2: The needle like structure used by Y. pestis to inject virulence factors into host cells.
Figure 2: The needle like structure used by Y. pestis to inject virulence factors into host cells.
Prevention:
Contact with dead or infected animals, especially rodents, should be avoided.
Treatment:
Commonly prescribed antibiotics for enterobacteria can be used to treat Y. pestis infections. CDC recommends that the treatment should begin as soon as plague is suspected. The earlier the treatment starts, the greater chance for patients to survive. Gentamicin and streptomycin are often prescribed as first line treatments due to their ability to stop the bacteria from making proteins it requires and to induce bacterial death. However, patients should not maintain on streptomycin for more than full 10 days in order to avoid the risk of developing endotoxic shock. They should gradually change to other antibiotics to continue the treatment. Treatments can be adjusted depending on the patient’s age, medical history and underlying health conditions as well.
WHO does not recommend vaccination against Y. pestis infections for general populations. However, for those who are often exposed to the risk of contamination and for health care workers, vaccinations should be considered.
Reference:
Auerbach, R. K., Tuanyok, A., Probert, W. S., Kenefic, L., Vogler, A. J., Bruce, D. C., … & Wagner, D. M. (2007). Yersinia pestis evolution on a small timescale: comparison of whole genome sequences from North America. PLoS One, 2(8), e770.
Galimand, M., Carniel, E., & Courvalin, P. (2006). Resistance of Yersinia pestis to antimicrobial agents. Antimicrobial agents and chemotherapy, 50(10), 3233-3236.
Li, B., & Yang, R. (2008). Interaction between Yersinia pestis and the host immune system. Infection and immunity, 76(5), 1804-1811.
Perry, R. D., & Fetherston, J. D. (1997). Yersinia pestis–etiologic agent of plague. Clinical microbiology reviews, 10(1), 35-66.
Plague.(2015,September 14). Retrieved November 20, 2017, from https://www.cdc.gov/plague/ prevention/index.html
Plague. (n.d.). Retrieved November 20, 2017, from http://www.who.Int/mediacentre/factsheets/ fs267/en/
