
by Sereena Moore
Introduction
Campylobacter jejuni is a gram-negative bacteria that causes gastroenteritis in humans. C. jejuni was first isolated in 1972. Since then, it has been known to be one of the main causes of gastroenteritis in the world. It is part of the gut microbiota of many animals including chickens, cattle, goats, dogs, ducks and pigs. However, it causes infection in humans by colonizing the intestinal tract.
Disease
The disease that results from infection by C. jejuni is called Campylobacteriosis. The most common ways that C. jejuni is transmitted is by consuming raw meat, poultry, contaminated water, unpasteurized milk or contacting contaminated animals (Figure 1). Symptoms of the infection are inflammation, watery/bloody diarrhea, fever, weight loss and abdominal cramps.

Figure 1: The most common modes of transmission of Campylobacter jejuni to humans. Source: Sereena Moore.
C. jejuni infection is also linked to other diseases. Some gastrointestinal disorders that may occur after infection are irritable bowel syndrome, pancreatitis, gastrointestinal hemorrhage, functional dyspepsia, and cholecystitis. Furthermore, infection is also connected to diseases in other parts of the body such as Guillain-Barre syndrome, Miller Fisher syndrome, meningitis, bacteremia, sepsis, arthritis, and endocarditis. These happen most often in young children, elderly or those who are immunocompromised. Guillain-Barre syndrome (GBS) is the most common, where 40% of people with GBS were previously infected by C. jejuni. GBS is a neurological condition where antibodies attack the myelin sheath, which is an insulting layer that covers peripheral nerves. Symptoms include limb weakness, problems with respiratory and cranial muscles and even paralysis. GBS and C. jejuni infections are hypothesized to be linked because structures on C. jejuni and proteins from the myelin sheath are structurally similar. Thus, antibodies in the host that were produced against C. jejuni begin to attack the myelin sheath and cause demyelination of the nerve.
Epidemiology:
Campylobacteriosis affects people all over the world. The first infection was officially recorded in the 1980s. Currently, C. jejuni is the cause of gastroenteritis in about 400-500 million people in the world each year. It is the most common disease that causes diarrhea, and studies show that it happens more often than infections from other pathogens, such as Salmonella, Shigella, and E. coli. Infections have recently increased in developed countries in North America, Europe and Australia. About 2.5 million people are infected with C. jejuni each year in the United States. In developing countries, infections from C. jejuni are more common in young children. The infection is also more common to those who are immunodeficient, especially those who have HIV. Outbreaks do not happen often, however, they can occur in places where many people have ingested raw milk or contaminated water.
Virulence:
Currently, the virulence factors used by C. jejuni are not completely understood. However, some mechanisms are known. First, C. jejuni has flagella, which are structures that aid in movement through the gastrointestinal tract, colonization and invasion of the gastrointestinal epithelial layer. The flagella are made up of amino acids that are modified by O-linked glycosylation, which is an addition of a carbohydrate onto the oxygen molecule of an amino acid. This modification is necessary during the assembly of the flagella and has shown to be crucial in the flagella’s functions of movement, colonization and invasion of host cells. Moreover, C. jejuni has a spiral shape that it also uses, along with the flagella, to pass through and invade the mucosa layer of the intestine (Figure 2). Once in the intestine, C. jejuni must bind to the epithelial layer to colonize the hosts intestine, using structures called adhesins. Finally, C. jejuni secretes a toxin called cytolethal distending toxin (CDT). CDT can either stop the hosts cell cycle during replication, or cause programmed cell death. It also helps trigger a response from the host immune system resulting in the release of interleukin-8, which is a cytokine released to induce inflammation and attract immune cells to the area.
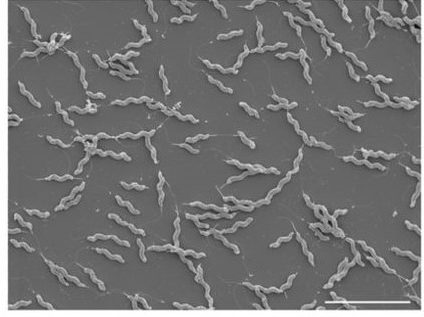
Figure 2: Scanning electron micrograph of the spiral shape and flagella of Campylobacter jejuni. It uses its spiral shape, and flagella to pass through the mucosa and epithelial cells of the humans’ intestine, for chemotaxis and adhesion. Source: Esson et al. 2016. Genomic variations leading to alterations in cell morphology of Campylobacter spp. Nature Scientific Reports. 6. https://www.nature.com/articles/srep38303#f1
Treatment:
Normally, treatment for C. jejuni infection is not required, as the infection normally goes away by itself. However, there are a few different treatment options. Fluid replacement may be used because of the large amount of water lost due to the diarrhea. Furthermore, antibiotics may be needed in some cases, such as for those who have severe symptoms, or who are immunocompromised. C. jejuni is known to be resistant to different types of antibiotics including quinolones, cloxacillin, vancomycin and B-lactams. Resistance is hypothesized to be occurring due to the usage of these antibiotics in veterinary medicine, especially in poultry. However, macrolides, such as erythromycin and azithromycin, have shown to be successful in treating serious cases of Campylobacteriosis. Macrolides interrupt protein synthesis in the bacteria, which causes them to stop growing.
Preventative measures are currently being taken to control the transmission of C. jejuni. These include preventing the spread of C. jejuni between chickens, the use of antimicrobial peptides in chickens to kill bacteria, vaccines and safer food handling practices at the slaughterhouse and processing.
References:
Acheson D, Allos BM. (2001). Campylobacter jejuni Infections: Update on Emerging Issues and Trends. Clinical Infection Diseases. 32(8):1201-1206. DOI: 10.1086/319760.
Altekruse SF, Stern NJ, Fields PI, Swerdlow DL. (1999). Campylobacter jejuni – An Emerging Foodborne Pathogen. Emerging Infecious Diseases. 5(1): 28-35. DOI: 10.3201/eid0501.99010
Dasti JI, Tareen AM, Lugert R, Zautner AE, Gross U. (2010). Campylobacter jejuni: A brief overview on pathogenicity-associated factors and disease-mediating mechanisms. International Journal of Medicl Microbiology. 300(4): 205-211. DOI: 10.1016/j.ijmm.2009.07.002.
Deun KV, Haesebrouck F, Heyndrickx M, Favoreel H, Dewulf J, Ceelen L, Dumez L, Messens W, Leleu S, Immerseel FV, Ducatelle R, Pasmans F. (2007). Virulence properties of Campylobacter jejuni isolates of poultry and human origin. Journal of Medical Microbiology. 56: 1284-1289. DOI: 10.1099/jmm.0.47342-0
Esson D, Mather AE, Scanlan E, Gupta S, de Vries SPW, Bailey D, Harris SR, McKinley TJ, Meric G, Berry SK, Mastroeni P, Sheppard SK, Christie G, Thomson NR, Parkhill J, Maskell DJ, Grant AJ. (2016). Genomic variations leading to alterations in cell morphology of Campylobacter spp. Nature Scientific Reports. 6. DOI: 10.1038/srep38303
Fouts DE, Mongodin EF, Mandrell RE, Miller WG, Rasko DA, Ravel J, Brinkac LM, DeBoy RT, Parker CT, Daugherty SC, Dodson RJ, Durkin AS et al. (2005). Major Structural Differences and Novel Potential Virulence Mechanisms from the Genomes of Multiple Campylobacter Species. PloS Biology. 3(1): e15. DOI: 10.1371/journal.pbio.0030015
Kaakoush NO, Castano-Rodriguez N, Mitchell HM, Man SM. 2015. Global Epidemiology of Campylobacter Infection. Clinical Microbiology Reviews. 28(3): 687-720. DOI: 10.1128%2FCMR.00006-15.
Ternhag A, Asikainen T, Giesecke J, Ekdahl K. 2007. A Meta-Analysis on the Effects of Antibiotic Treatment on Duration of Symptoms Caused by Infection with Campylobacter Species. Clinical Infectious Diseases. 44(5): 696-700. DOI: 10.1086/509924
Young KT, Davis LM, DiRita VJ. 2007. Campylobacter jejuni: molecular biology and pathogenesis. Nature Reviews Microbiology. 5: 665-679. DOI: 10.1038/nrmicro1718.
